

You may never have given it much thought but have you ever considered how truly awesome the human heart is? When healthy and strong, this chest organ pumps blood with cell-nourishing oxygen through all the nooks and crannies (veins and capillaries, that is) inside our bodies.
The human heart has two chambers, the left atrium, and the right atrium. Within the right atrium resides the sinoatrial [SI-no-A-tree-al] node, a small bundle of specialized cells, which is known as the heart’s natural pacemaker. The SA node kicks off the normal cardiac cycle, generating an electrical impulse that travels right through the walls of the atria, causing them to contract.
Then, a cluster of cells in the center of the heart between the atria and ventricles called the atrioventricular [A-tree-o-ven-TRICK-you-lar] node functions delays the electrical signal before it enters the ventricles, giving the atria time to contract before the ventricles do.
Finally, the His–Purkinje system, a pathway of fibers, sends the impulse to the muscular walls of the ventricles, causing them to contract.
The SA node sparks another electrical impulse to start the cycle again, keeping the heart beating and blood flowing inside the body.
The normal resting heart rate for adults ranges from 60 to 100 beats per minute (bpm). In general, the lower the resting heart rate a person has, the healthier that person is.
A heart rate that is unusually high or low or irregular may signal an underlying medical problem. A consistent pulse of 100 bpm is termed tachycardia whereas a resting heart rate below 60 bpm (except for athletes) is called bradycardia.
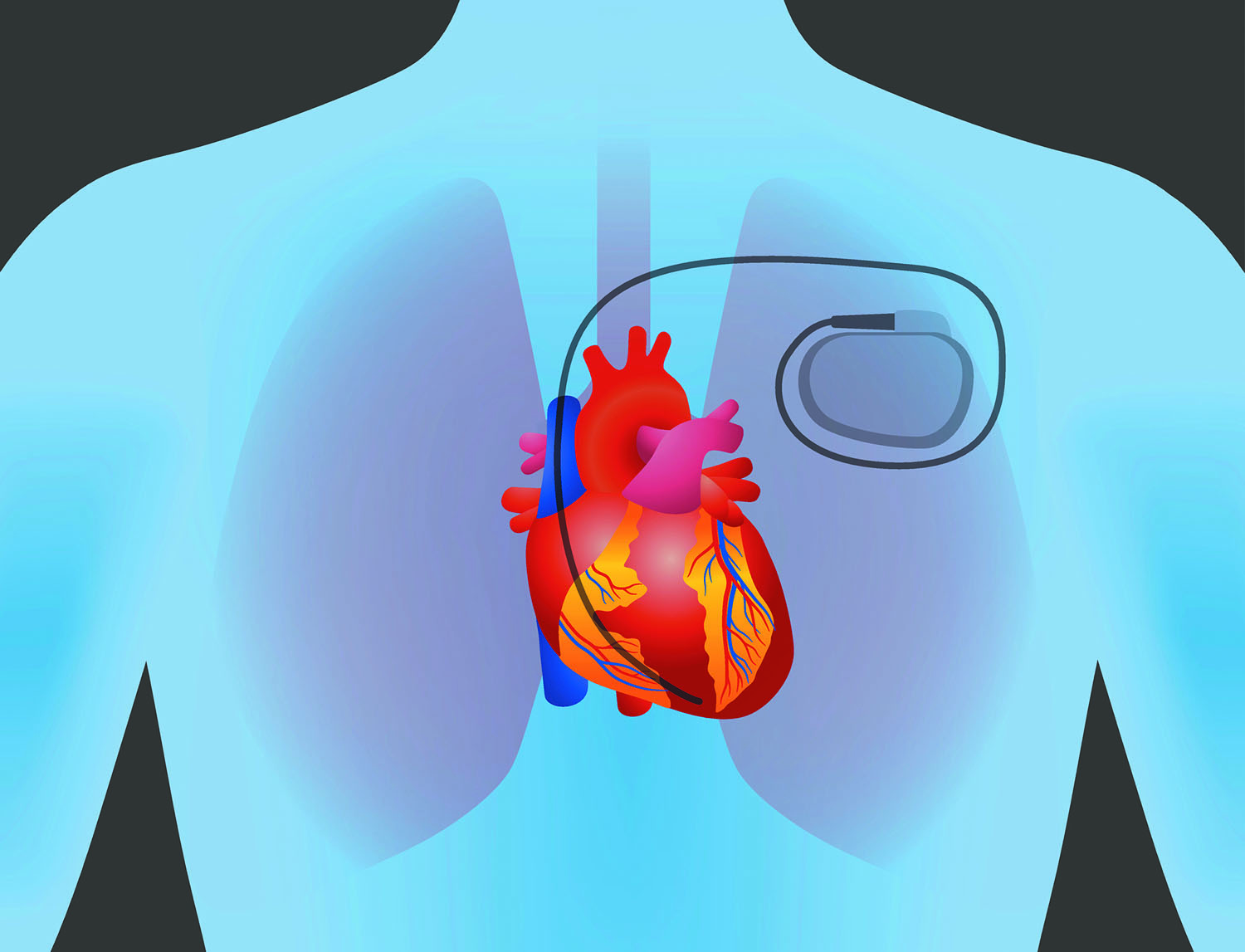
Some heart disorders develop as a consequence of aging, cardiac damage from a heart attack or from other conditions that interfere with the heart’s electrical activity. In such cases, doctors often recommend a prosthetic assistant, an electronic device that helps the heart beat at the proper rhythm: a pacemaker.
Pacemakers are commonly used to treat bradycardia, atrial fibrillation (a type of arrhythmia), syncope (fainting due to low heart rate), and heart block, a disorder that occurs if an electrical signal is slowed or disrupted as it moves through the heart.
Heart disorders can be identified with an electrocardiogram (EKG or ECG) which is a simple, painless test where a technician attaches electrodes on the patient’s body that detect and record the heart’s electrical activity on graph paper. The test captures heart rate, rhythm (steady or irregular), and the strength and timing of electrical signals as they pass through the heart muscle.
Internal pacemakers to regulate cardiac pacing (heart rate) have been around awhile. Dr. Rune Elmqvist performed the first successful pacemaker transplant operation at the Karolinska University Hospital in Solna, Sweden, on October 8, 1958.
These days, about 200,000 pacemakers are implanted annually in the U.S. They provide transcutaneous pacing (also called external pacing) via electrical cardiac stimulation to treat an abnormal heart rate. The purpose of cardiac pacing is to re-establish circulatory integrity and normal hemodynamics
Pacemakers haven’t changed much since they were introduced. The technology is straightforward: two electrodes attached to the pacemaker emit electrical signals to stimulate the heart muscles, causing them to begin contractions when they stop working.
A modern pacemaker only has two parts – a power source (generator or battery) and connecting wires (electrical leads). The very small device, which weighs about one ounce and is about the size of a large watch face, can be surgically implanted in the chest under the skin.
Single-chamber pacemakers have a lead to only one of the heart’s chambers, while dual-chamber pacemakers have two leads that connect to two chambers.
Pacemakers rely on their electrical leads to monitor the heart’s rate and rhythm non-stop. They can deliver either small electrical pulses or larger jolts as needed.
Pacemaker leads can malfunction or stop working completely from damage caused by the patient’s bending and flexing, which can sever, twist or dislodge the leads.
Often, it isn’t easy to remove an implanted pacemaker. The fibrous scar tissue that can grow around the wire and adhere to it. Some experts recommend leaving non-functional leads inside the body rather than removing them, advising extraction only for infected pacing or defibrillation systems.
Surgeons can use lasers to cut away the scar tissue but another solution is the leadless pacemaker, first proposed in the 1970s, which is inserted in the right ventricle of the heart.
The leadless pacemaker is the size of a dime, free-standing, and inserted via femoral venous access where it is attached to the right ventricular myocardium and released. The delivery system is then removed and the pacemaker remains embedded in the right ventricle.
The advantages of a pacemaker with no hard-wired electrical leads include:
- No lump at the implant site
- A shorter procedure which uses a catheter for insertion
- No limits to upper body motion post-implant
The Food and Drug Administration (FDA) approved Medtronic’s Micra leadless pacemakers in April 2016.
Worldwide, the leadless cardiac pacemakers market is projected to grow from $47 million in 2017 to just under $270 million by 2026.
Medical device manufacturers actively participating in the leadless cardiac pacemakers market are Boston Scientific Corporation, EBR Systems, Inc., Medtronic, Plc., Nanostim, Inc., and St. Jude Medical, Inc.
Revolutionary leadless pacemakers are considered a safe alternative for patients who require single-chamber pacing. Recipients of leadless cardiac pacemakers report superior features such as extended battery life, minimal post-implantation complications, and no device dislodgement in comparison to traditional pacemakers.
